Background on the Medicare Drug Price Negotiation Program, Effectuation of Maximum Fair Prices (MFPs)

Compliance Corner with IPA: Reimbursement cuts in 2026
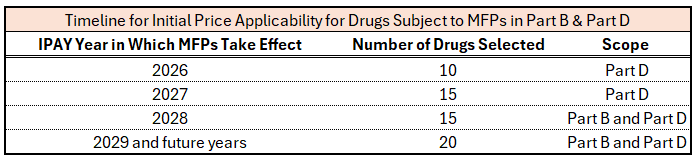
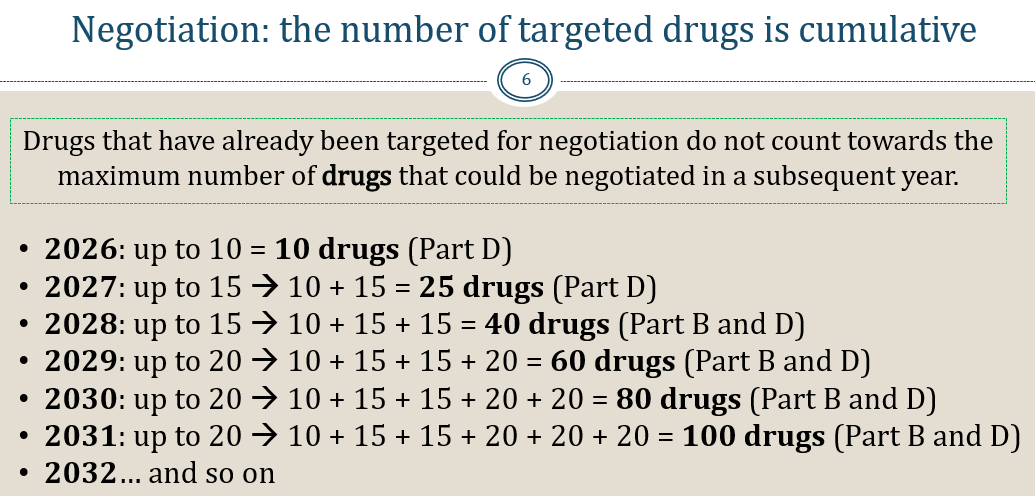
The Inflation Reduction Act (IRA), signed into law in 2022, created the Medicare Drug Price Negotiation Program (MDPNP). The law provides Medicare the ability to directly negotiate the prices of certain high expenditure, single source drugs without generic or biosimilar competition. Negotiated prices are referred to as Maximum Fair Prices (MFPs). Manufacturers that fail to come to an agreement with the Secretary are liable for a 1900% tax on all U.S. sales of that product or risk exclusion of all the company’s portfolio of products from all government programs. MFPs are applicable to Part D and Part B drugs. MFPs are effectuated for initial price applicability years (IPAY) 2026 and 2027 for Part D drugs only. On January 1, 2028, and in future years, MFPs will apply to Part D and Part B drugs as detailed in the graphic below. Part B drugs selected for the MDPNP for IPAY 2028 will be announced by February 2026. The Congressional Budget Office (CBO) originally projected MFP prices would fall “roughly 50%,” but revised its projection to 25-50% in 2024.
MFP + 6% versus ASP + 6% Reimbursement Methodology Threatens Provider Viability & Patient Access to Community Based Infusion Providers
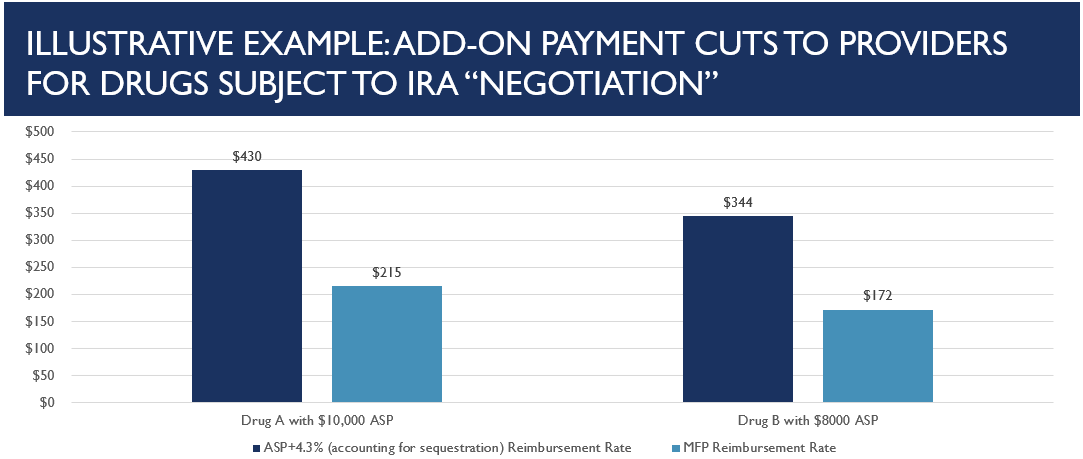
An unintended consequence of the MDPNP threatens provider viability and patient access to Infusion Providers Alliance (IPA) member clinics and physician offices and many of Infinity Infusion Solutions’ clients who administer Part B drugs. When an MFP is instituted for a Part B drug, Medicare’s add-on payment for administration of the drug will fall from average sales price (ASP) + 6% to MFP + 6%. Because providers who administer drugs in Part B rely on the add-on payment as their principal revenue stream for drug administration, due to insufficient professional fees only covering a fraction of provider’s costs, a 50% cut to their primary reimbursement represents a severe threat to provider viability and patient access. An illustrative example of cuts to providers for drugs subject to negotiation is detailed below.
MFP + 6% versus ASP + 6% Reimbursement Methodology Threatens Provider Viability & Patient Access to Community Based Infusion Providers
An unintended consequence of the MDPNP threatens provider viability and patient access to Infusion Providers Alliance (IPA) member clinics and physician offices and many of Infinity Infusion Solutions’ clients who administer Part B drugs. When an MFP is instituted for a Part B drug, Medicare’s add-on payment for administration of the drug will fall from average sales price (ASP) + 6% to MFP + 6%. Because providers who administer drugs in Part B rely on the add-on payment as their principal revenue stream for drug administration, due to insufficient professional fees only covering a fraction of provider’s costs, a 50% cut to their primary reimbursement represents a severe threat to provider viability and patient access. An illustrative example of cuts to providers for drugs subject to negotiation is detailed below.
CMS’s CY 2026 Physician Fee Schedule (PFS) Final Rule Exacerbates MFP/ASP Concerns
In the CY 2026 PFS final rule, CMS finalized policy on the calculation and reporting of ASP as it relates to MFP. Despite strong objections from IPA and many others, CMS adopted proposals to:
⦁ Allow MFPs to flow into and influence the calculation of ASP for drugs selected for negotiations
⦁ Replace the market-based ASP drug pricing file entirely with an MFP-only file
Because ASP is the predominant benchmark used by commercial payers in contracts for provider-administered medications, replacing ASP with the substantially lower MFP price will have a devastating impact on providers’ ability to deliver medications subject to negotiation to commercially insured patients. The “underwater biosimilars” challenge unfortunately provides a real world example of what could happen when providers are put substantially underwater and cannot administer products without taking a substantial loss. Over time, as more drugs come into negotiation, the long-term viability of non-hospital, community-based infusion providers will be severely threatened as, by definition, these drugs are the most economically significant.
Legislative Solution: Enact HR 4299, the Protecting Patient Access to Cancer and Complex Therapies Act
IPA’s top legislative priority, HR 4299, would protect providers and their patients from collateral damage in negotiations between CMS and manufacturers. Major components of the bill, which currently has 16 bipartisan sponsors in the House of Representatives, include:
⦁ Providers continue to be reimbursed at pre-IRA ASP + 6% levels on drugs subject to negotiations and MFPs
⦁ Beneficiary coinsurance continues to be based off lower MFP prices
⦁ Manufacturers pay a rebate to CMS to account for the provider payment differential, ensuring savings
⦁ MFPs are prohibited from influencing and artificially eroding the calculation of ASP
IPA is working with a broad coalition of stakeholders to generate further bipartisan support and Congressional action on this critical legislation. To learn more about this work and how you can get involved in these and other IPA advocacy efforts, please contact ewarren@infusionprovidersalliance.org or visit our website.
About the Infusion Providers Alliance (IPA)
IPA represents community-based, non-hospital affiliated independent ambulatory infusion clinics and physician practices that deliver complex biologic infused or injected therapies to patients at the lowest cost, clinically appropriate setting of care. Our members operate over 1,000 community-based, non-hospital sites across 46 states. These sites of service are strategically located in the communities where patients live and work. They provide patients with flexibility and convenience when receiving treatment for conditions such as Crohn’s disease, ulcerative colitis, multiple sclerosis, rheumatoid arthritis, and many other chronic, complex, and rare conditions and do so with a level of clinical excellence that studies have shown to be superior to any other setting of care. IPA members are committed to preserving the integrity of the provider-patient relationship in a manner that delivers exceptional care to patients and value to the health care system.